
AI in Hospital Management System: From Record Keeping to Clinical Intelligence
For most of its history, a Hospital Management Information System has done one thing well: store.
It has captured patient demographics, logged consultations, recorded prescriptions, tracked billing, and archived lab results. Done well, it has made that information retrievable - faster than a paper file, more organized than a cabinet drawer, accessible from more than one desk at a time.
That was genuinely useful. It still is.
But storage is not intelligence. A system that holds data and a system that thinks with data are two fundamentally different things - and healthcare is arriving, now, at the moment where the second kind becomes possible at scale.
The question for every hospital, clinic, and health system is not whether AI will change what a hospital information system does. It will. The question is whether they will understand what is changing well enough to make good decisions about it.
This is an attempt to explain it clearly.
The Four Technologies Driving the Shift
Before exploring what an AI-enabled HMIS does differently, it's worth understanding the four underlying technologies making it possible. These are not interchangeable terms. They do different things, and they are most powerful when they work together.
Large Language Models (LLMs)

A Large Language Model is an AI system trained on vast quantities of text - medical literature, clinical guidelines, research papers, drug references, patient record formats - that develops the ability to understand and generate human language with remarkable fluency and contextual awareness.
In a healthcare context, an LLM can read a clinician's free-text notes and extract structured information from them. It can interpret a patient's reported symptoms and map them to clinical concepts. It can understand that "Nairobi" and "Nbi" in two patient records likely refer to the same thing, and that a complaint of "kichwa kuuma" and "headache" describe the same symptom in different languages.
LLMs are the comprehension engine. They are what allows an AI system to understand the meaning behind clinical data, not just its format.
Retrieval-Augmented Generation (RAG)
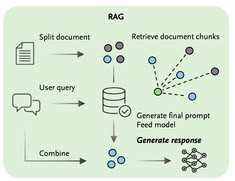
One limitation of a standalone LLM is that its knowledge is bounded by its training data. A model trained up to a certain date doesn't know about guidelines published since. A general-purpose model may not have been trained on the specific drug formulary used in Kenya, or the locally-adapted clinical protocols relevant to a particular facility or disease context.
Retrieval-Augmented Generation solves this by giving the LLM the ability to search, in real time - a curated, trusted knowledge base before generating a response. That knowledge base might include current WHO guidelines, national treatment protocols, a facility's approved formulary, past anonymized cases, or specialist literature.
The combination is powerful: the LLM provides reasoning and language capability; the RAG layer provides current, verified, locally-relevant facts. The result is a system that doesn't just know a lot - it knows the right things, in context, at the moment of need.
Agentic AI

An AI agent is a system that doesn't just respond to a question, it takes initiative. It can observe a situation, determine what action is needed, execute that action, observe the result, and continue until a defined goal is achieved.
In a passive AI system, a clinician asks a question and the system answers. In an agentic system, the AI monitors the workflow continuously, identifies moments where intervention adds value, and acts - flagging a duplicate patient record before it causes a billing error, auto-populating a radiology request based on the clinical notes already in the system, generating a safety alert the moment a dangerous drug combination is prescribed.
Agentic AI is the difference between a system that answers when spoken to and one that actively participates in the work.
Explainable AI (XAI)
In healthcare, an AI recommendation that cannot be explained is an AI recommendation that should not be trusted. Clinicians - and patients, and regulators - need to understand not just what the AI is suggesting but why.
Explainable AI refers to the design of AI systems so that their reasoning is transparent and interpretable by a human. When an AI flags a drug interaction, XAI allows the system to show the clinician exactly which drug combination triggered the alert, what the mechanism of interaction is, and what the evidence behind that concern says. When a differential diagnosis is suggested, XAI displays which clinical findings contributed to that ranking and with what weight.
This transparency is not just an ethics requirement. It is the mechanism through which clinical trust in AI recommendations is built and maintained. A clinician who can see why the system is saying what it's saying can make an informed decision about whether to follow, modify, or override the suggestion, and that clinical judgment remains exactly where it belongs.
What This Looks Like Across the Patient Journey
When LLMs, RAG, Agentic AI, and XAI are woven together inside a hospital management system, the entire patient journey changes. Not dramatically at any single point - but cumulatively, in ways that add up to a fundamentally different clinical experience.
Here is what that looks like, step by step.
Step 1: Patient Registration - No More Duplicate Records
The problem today: A patient registers at your facility. Their name is spelled slightly differently from how it was captured on a previous visit. They give a different phone number. The system creates a second record. Over months and years, your database accumulates thousands of fragmented patient histories - clinical decisions being made against incomplete records, billing going to wrong contacts, lab results attached to the wrong file.
What AI changes: When a new patient is entered, an LLM interprets variations in name spelling, address formats, and demographic combinations to identify potential matches with existing records. An Agentic AI component autonomously evaluates the similarity, merges confirmed duplicates, and flags uncertain cases for human review - before the second record is ever saved.
The outcome is a single, clean Master Patient Record from the first interaction. Clinical decisions downstream are made against complete information. And the administrative burden of deduplication, currently a manual, time-consuming process in most facilities - disappears.
Step 2: Triage - Dynamic Risk Assessment, Not Static Screening
The problem today: A nurse records a patient's vitals at triage: temperature, blood pressure, heart rate, oxygen saturation, respiratory rate. The numbers are documented. Whether they constitute a pattern that warrants urgent escalation depends on the clinical experience and attention of whoever is reading them - which varies by shift, by staffing level, and by how busy the queue is.
What AI changes: As vitals are entered, an LLM augmented by RAG pulls the patient's relevant history - prior admissions, known conditions, recent lab results - and cross-references it against clinical guidelines for the presenting combination of findings. The system generates a dynamic risk score: not just a number, but a structured summary of what's driving it.
If the combination of a slightly elevated temperature, a rising heart rate, and a recent surgical wound suggests early sepsis rather than a routine post-operative fever, the system flags it, with an explanation, before the patient has moved from the triage chair to the waiting area.
Early warning doesn't require a specialist at triage. It requires a system that recognizes patterns at a scale no individual can match.
Step 3: Consultation - The End of the Documentation Burden
The problem today: Across the world, clinicians spend a disproportionate amount of their consultation time on documentation rather than the patient in front of them. In African healthcare settings where a doctor may see 40 to 60 patients in a session, the cognitive and administrative load of maintaining detailed clinical records is often what gets sacrificed first. Notes become abbreviated. Important context gets omitted. The quality of the record degrades under pressure.
What AI changes: Agentic AI acts as a digital clinical scribe. During the consultation, it listens - or processes typed notes in real time - and structures the interaction into a formal SOAP note: Subjective (what the patient reports), Objective (what the clinician observes and measures), Assessment (the clinical interpretation), Plan (the intended management).
It handles translation where needed. It identifies clinical terminology from conversational language. And it drafts the structured note automatically, requiring the clinician only to review and confirm
The consultation refocuses on the patient. The documentation happens in the background. The record that results is more complete, more structured, and more useful to the next clinician who reads it.
Step 4: Diagnosis - A Second Opinion That Has Read Everything
The problem today: Diagnostic accuracy depends heavily on clinical experience and access to current medical knowledge. A generalist seeing an unusual presentation may not recall the relevant literature. A junior clinician may not yet have the pattern recognition that comes with years of practice. And in facilities where specialist support isn't immediately accessible, difficult cases can sit without adequate guidance.
What AI changes: After the clinician inputs their clinical findings, a RAG-enhanced LLM cross-references them against a curated knowledge base - current clinical guidelines, indexed medical literature, locally-validated case data - and returns a ranked differential diagnosis.
Explainable AI then does something critical: it shows the clinician exactly which clinical findings contributed to each ranked diagnosis, and on what evidence basis. The system isn't saying "it might be X." It's saying "based on the three-day fever, the hepatosplenomegaly, and the travel history to a malaria-endemic region, the primary consideration is plasmodium falciparum malaria - here is the guideline reference supporting this."
The clinician retains full decision-making authority. But they are making that decision with access to reasoning that extends well beyond any single person's expertise.
Step 5: Diagnostic Ordering -The Right Test, Not the Reflex Test
The problem today: Over-investigation is a significant and underacknowledged problem in healthcare. Partly it reflects clinical uncertainty - when you don't know what you're looking for, you order broadly. Partly it reflects habit. Partly it reflects the absence of any real-time guidance on what is and isn't appropriate for a given clinical presentation.
The consequence is unnecessary cost to patients, delays in reaching the right diagnosis, and inefficient use of diagnostic resources that are already stretched.
What AI changes: Based on the structured clinical notes, an Agentic AI component consults a RAG-powered knowledge base of appropriateness criteria - locally-adapted guidelines for which investigations are indicated in which clinical contexts. It recommends the most clinically appropriate and cost-effective test for the presentation. Where a radiology investigation is indicated, it auto-populates the imaging request with the correct protocol.
The clinician can accept, modify, or override the recommendation. But the default - the path of least resistance - is now the appropriate investigation rather than the reflexive one.
Step 6: Prescribing - Safety Checks That Never Get Tired
The problem today: Medication errors are one of the most preventable causes of patient harm in healthcare. Allergies that were documented but not checked. Drug combinations that interact dangerously. Doses that are appropriate for a healthy adult but contraindicated in the presence of renal impairment. In a busy prescribing environment, these checks depend on human vigilance, which fluctuates.
What AI changes: As a prescription is ordered, Agentic AI runs simultaneous checks against the patient's documented allergy record, their current medication list, and their relevant clinical parameters. It checks for drug-to-drug interactions, allergy contraindications, dose appropriateness given renal or hepatic function, and age-specific safety thresholds, in seconds.
If a risk is detected, the system generates an alert with a hard stop, the prescription cannot be finalized until the clinician actively responds. Explainable AI displays exactly what triggered the alert: which allergy, which interaction, which clinical value, and what the evidence says about the risk level.
The clinician can override with documented clinical reasoning. What they cannot do is proceed without knowing. The safety net is not optional.
The Shift That Is Already Underway

The movement from systems of record to systems of intelligence is not a future trajectory, it is happening now. The question for hospital leadership and health system decision-makers is not whether to engage with it, but how to engage with it well.
It means building clinical cultures that are prepared to work with AI recommendations - not blindly following them and not reflexively ignoring them, but engaging with them as a skilled professional engages with any tool: understanding its strengths, knowing its limitations, and applying judgment at every step.
And it means working with technology partners who are building AI into healthcare systems with the same seriousness they bring to clinical accuracy - investing in local data validation, designing for clinical workflows in the specific environments where the system will be used, and treating clinician trust as a design requirement, not an afterthought.
At Hanmak Technologies, this is the direction in which MedicentreV3 is evolving. Not toward a system that replaces clinical judgment, but toward one that earns the right to sit beside it.
The Bottom Line

The movement from systems of record to systems of intelligence is not a future trajectory, it is happening now. The question for hospital leadership and health system decision-makers is not whether to engage with it, but how to engage with it well.
It means building clinical cultures that are prepared to work with AI recommendations - not blindly following them and not reflexively ignoring them, but engaging with them as a skilled professional engages with any tool: understanding its strengths, knowing its limitations, and applying judgment at every step.
And it means working with technology partners who are building AI into healthcare systems with the same seriousness they bring to clinical accuracy - investing in local data validation, designing for clinical workflows in the specific environments where the system will be used, and treating clinician trust as a design requirement, not an afterthought.
At Hanmak Technologies, this is the direction in which MedicentreV3 is evolving. Not toward a system that replaces clinical judgment, but toward one that earns the right to sit beside it.





